Why I Have a Love-Hate Relationship With Janda’s Crossed Syndromes
There are a few concepts in the rehab and bodywork world that refuse to die. Upper Crossed Syndrome and Lower Crossed Syndrome are definitely on that list.
And honestly, I understand why.
They are simple. They are easy to visualize. They give practitioners a framework for understanding common postural and movement adaptations. And for a lot of therapists, early in their careers, they can feel like someone finally handed them a map to understanding some common postures we encounter.
But the longer I’ve worked with people, coached movement, studied pain science, and looked at the actual variability of human bodies, the more complicated my relationship with these syndromes has become. While Janda absolutely contributed valuable ideas to rehabilitation and movement science, I think many practitioners have taken these patterns far too literally. And when that happens, we stop assessing humans and start assessing templates.
First, Let’s Talk About What Janda Actually Proposed
Vladimir Janda was a Czech neurologist and physician who observed common muscular imbalances and movement adaptations in people with pain and dysfunction. The two most commonly discussed patterns are Upper Crossed Syndrome and Lower Crossed Syndrome.
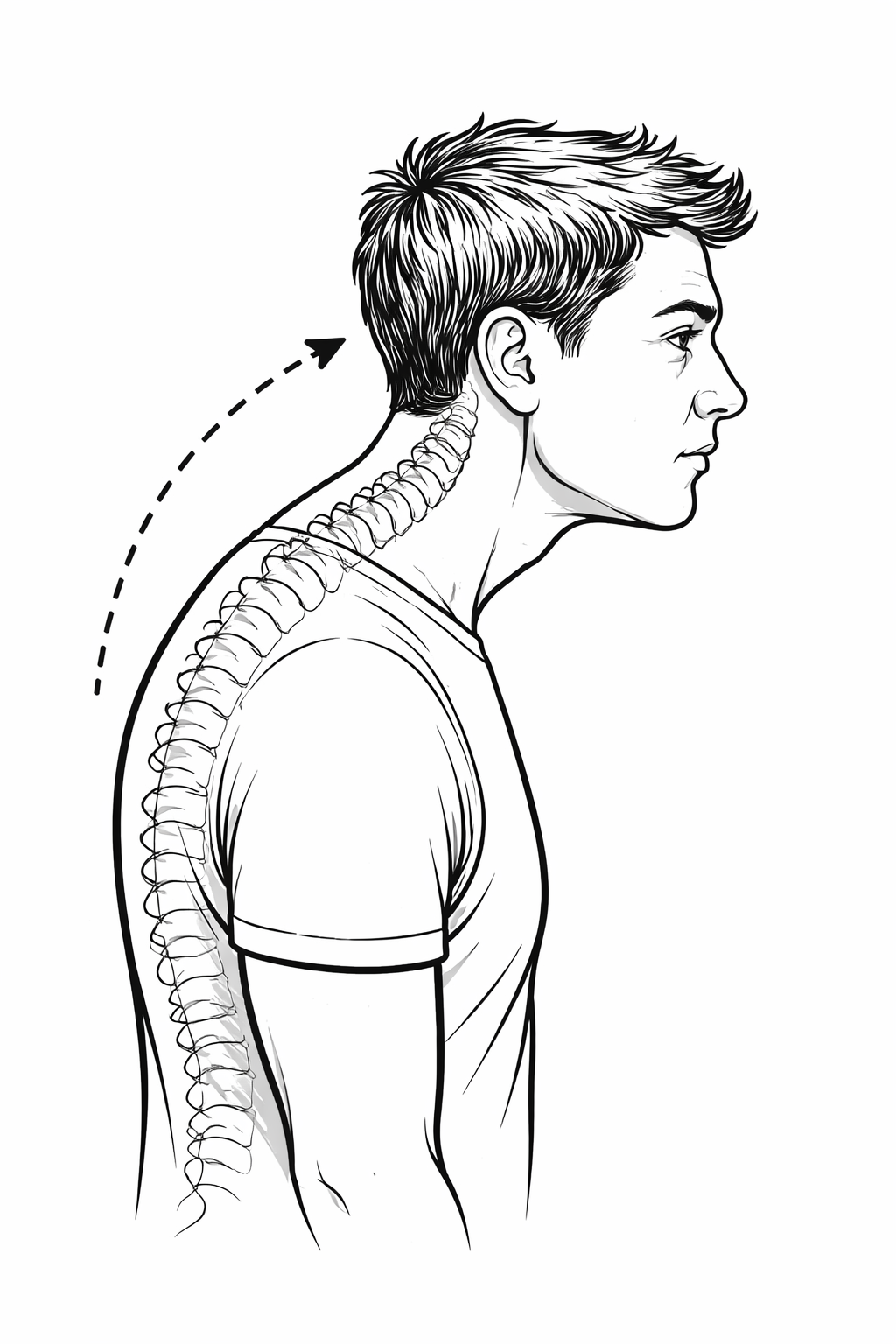
Upper Crossed Syndrome
Traditionally, Upper Crossed Syndrome describes a pattern where:
The upper trapezius, levator scapulae, and pectorals are considered short or overactive
The deep neck flexors and lower trapezius are considered inhibited or weak
Visually, this often gets associated with:
Forward head posture
Rounded shoulders
Increased thoracic kyphosis
Lower Crossed Syndrome
Lower Crossed Syndrome typically describes:
Tight or overactive hip flexors and lumbar extensors
Weak or inhibited abdominals and glutes
Which is commonly associated with:
Anterior pelvic tilt
Increased lumbar lordosis
Changes in gait and movement mechanics
And here’s the thing: These patterns absolutely can exist. People do develop predictable adaptations. Muscles do adapt to repetitive positions and loading strategies. Movement does become habitual. But somewhere along the way, the industry started treating these syndromes less like observations and more like laws of nature.
That’s where I start having issues.
Posture Is Not a Diagnosis
One of the biggest mistakes I see practitioners make is assuming posture automatically tells us what is tight, weak, dysfunctional, painful, or problematic. That leap is not supported nearly as strongly as people think. You cannot reliably look at someone standing still and determine:
Which muscles are truly weak
Which tissues are stiff
Which structures are painful
Which movement strategies are compensatory
Or whether the person even has a problem at all
We have people with “terrible posture” and zero pain. We also have people with beautiful textbook posture who hurt constantly. The difference between my girlfriend and I are a prime example of this. Most people would say my girlfriend has excellent posture, especially in the upper body, yet her most common complaint is neck and shoulder pain. While I have a pretty obvious forward head posture, and yet, I rarely have any neck pain.
Human bodies are adaptable. And adaptation is not automatically pathological. That difference matters. A forward head posture does not automatically mean the deep neck flexors are weak. An anterior pelvic tilt does not automatically mean the glutes are shut off. Rounded shoulders do not automatically mean someone needs pec release and band pull-aparts. Sometimes those interventions help, and sometimes they do absolutely nothing. Sometimes they may even make things worse because we never identified the actual limitation in the first place.
Short Does Not Always Mean Tight
This is another area where I think people get into trouble. A muscle being in a shortened position does not automatically mean it is adaptively shortened. Likewise, a muscle being lengthened does not automatically mean it is weak.
Those are assumptions, and assumptions can be dangerous in assessment.
For example, someone may appear to have tight hip flexors because they stand in anterior pelvic tilt, but when you actually assess hip extension, maybe they have plenty of mobility. Maybe the issue is motor control. Maybe it is a stability strategy. Maybe it is breathing mechanics. Maybe it is load tolerance. Maybe they simply spend eight hours a day sitting, and their nervous system defaults to a familiar resting posture.
That does not necessarily mean their psoas needs to be aggressively smashed into oblivion. The same goes for thoracic kyphosis and rounded shoulders. Sometimes the thoracic spine is actually stiff. Sometimes it is not. Sometimes the person lacks upward rotation. Sometimes they lack strength overhead. Sometimes they are just structurally built that way.
You do not know until you assess.
The Body Is Not a Collection of Isolated Muscles
One thing I appreciate about Janda’s work is that it tries to look at the body as an integrated system. That’s important because dysfunction rarely exists in isolation. But ironically, many modern interpretations of crossed syndromes became incredibly reductionistic. People memorize patterns: Tight pecs, weak lower traps, tight hip flexors, weak glutes.
And then treatment becomes a protocol instead of clinical reasoning: Release this, strengthen that, stretch this, activate that.
But human movement is far more dynamic than that. The nervous system organizes movement based on efficiency, safety, previous experience, available mobility, strength, fatigue, stress, injury history, and environmental demand, just to name a few. The posture you see is often just the visible outcome of a much larger strategy. And if you only chase the visible posture, you may completely miss the reason the body adopted it.
We Need Better Assessment
This is why I care so much about movement assessment. Not performative assessments, not arbitrary corrective exercise checklists, not fear-based posture analysis.
Actual assessment.
Can the person move? Can they control the movement? Do they have access to that range of motion? Do symptoms change under load? Can they dissociate segments? What happens when we change position? What happens when we alter breathing? What happens when we decrease threat or improve stability?
All that information matters far more than whether someone looks like a textbook Upper Crossed Syndrome chart from 1987.
The Industry Has Overpathologized Normal Adaptation
One of my bigger frustrations in rehab and bodywork education is how aggressively normal human variation gets pathologized. Not every kyphotic posture is a dysfunction, not every anterior pelvic tilt needs correction, and not every asymmetry is dangerous. Athletes adapt. Workers adapt. Humans adapt.
A powerlifter, swimmer, desk worker, gymnast, and jiu-jitsu athlete are all going to develop different movement tendencies. That is not automatically bad. Our job is not to force every person into the same idealized posture; our job is to improve function, capacity, tolerance, and quality of movement relative to the demands of that individual’s life. That is a completely different framework.
So, Are Crossed Syndromes Useless?
No.
I still think they can be useful as observational models. Patterns and being able to recognize patterns still matter. Humans absolutely develop predictable compensations, and Janda helped move rehabilitation toward the understanding that the body operates through coordinated systems rather than isolated tissues. That was immensely valuable, but crossed syndromes should be the beginning of your thinking. If you use them as rigid diagnostic categories, you will eventually miss what is actually happening in front of you. And if you automatically prescribe the same corrective exercises to every person who stands with an anterior pelvic tilt or rounded shoulders, you are no longer assessing. You are pattern matching, and those are not the same thing.
Final Thoughts
I think Janda’s work deserves respect, but I also think the rehab and fitness industries simplified his ideas into something much more rigid than they were intended to be. The body is adaptable, movement is contextual, and posture is variable, and good practitioners learn to ask better questions before jumping to conclusions.
So the next time you look at a client and think: “Upper Crossed Syndrome.” Pause for a second. Assess. Test your assumptions. Look at movement instead of just static posture. Because the body in front of you is always more complex than the chart in the textbook.